A clear guide to the differences between lifting a drooping brow and lowering a high hairline, including indications, techniques, recovery, risks and realistic expectations.
Important: This article is for general education and consultation support. It does not replace a personalised consultation with a suitably qualified surgeon. At MACS Clinic, the discussion includes the option of no surgery, non-surgical treatment where appropriate, and a realistic assessment of what surgery can and cannot achieve.
Forehead lift and forehead reduction are not the same operation
Patients often describe several different concerns as “forehead surgery”. In practice, there are two overlapping but distinct procedures. A forehead lift or brow lift primarily repositions the brow and upper-face soft tissues. A forehead reduction or hairline-lowering operation primarily reduces the vertical height of the forehead by bringing the frontal hairline forward.
Main purpose | Lift a low or heavy brow and soften upper-face heaviness. | Bring the hairline forward to reduce forehead height. |
Best for | Brow ptosis, tired appearance, forehead lines, lateral brow descent. | High forehead, long forehead proportion, stable hairline and good scalp laxity. |
Effect on wrinkles | May improve forehead and frown lines, depending on technique. | Usually limited effect on wrinkles unless combined with brow lifting. |
Effect on hairline | Some techniques may alter perceived forehead height. | Directly lowers the hairline. |
Upper-face anatomy in simple terms
The upper face includes the hairline, forehead skin, forehead muscles, eyebrows and upper eyelids. A heavy upper eyelid can be caused by excess eyelid skin, a drooping brow, or both. Correct diagnosis matters because removing eyelid skin alone may not correct a low brow.
Indications for a forehead / brow lift
Aesthetic indications
- Low or drooping eyebrows
- Heavy or tired-looking upper eyelids due to brow descent
- Deep horizontal forehead lines
- Vertical frown lines between the eyebrows
- Loss of lateral brow support
Functional indications
- Brow descent contributing to visual-field obstruction
- Forehead muscle fatigue from constantly lifting the brows
- Difficulty applying make-up because of upper-eyelid heaviness
Indications for forehead reduction / hairline lowering
Forehead reduction can be useful when the main concern is a high hairline rather than brow descent. It is particularly relevant in selected women with a naturally high forehead, good scalp mobility and a stable hairline. It is used more cautiously in men because future hairline recession may expose the scar or change the long-term aesthetic balance.
- High forehead disproportionate to the rest of the face
- Desire to bring the entire frontal hairline forward
- Stable hairline and no active progressive hair loss
- Adequate scalp laxity for safe advancement
Common surgical techniques
Technique selection depends on hairline, forehead height, skin quality, brow shape, sex-specific aesthetics, previous surgery and patient goals. No single technique is ideal for every patient.
Endoscopic brow lift
Small incisions are placed in the scalp and an endoscope assists release and elevation. It can be useful for mild-to-moderate brow descent, with relatively small scars. It may be less suitable for some patients with a high or receding hairline.
Pretrichial / hairline brow lift
The incision is placed at or close to the hairline. It can lift the brow while avoiding further lengthening of an already high forehead. Scar quality, hair direction and skin healing are important considerations.
Temporal / lateral brow lift
This focuses mainly on the outer brow. It can be useful for lateral hooding and may be combined with upper blepharoplasty in selected patients.
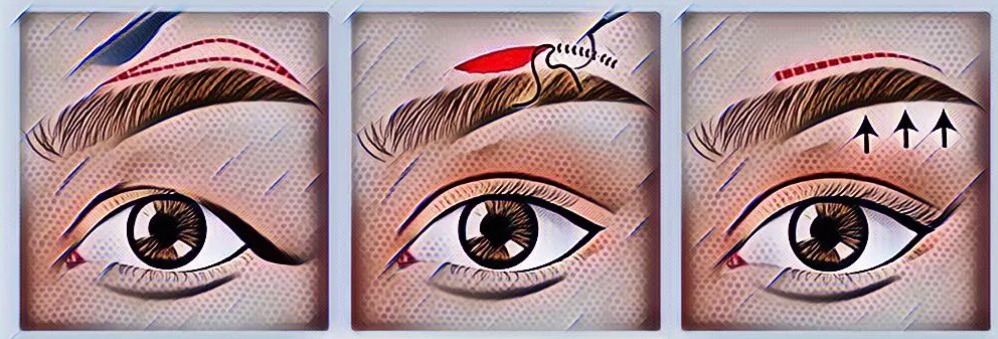
Direct brow lift
The incision is placed just above the eyebrow. It gives direct and precise control, often in functional or reconstructive situations, but the scar position must be carefully considered.
Coronal brow lift
A longer incision is hidden within the scalp. It can produce a powerful lift, but may not be suitable for patients with a high forehead or concerns about scalp sensation and hairline changes.
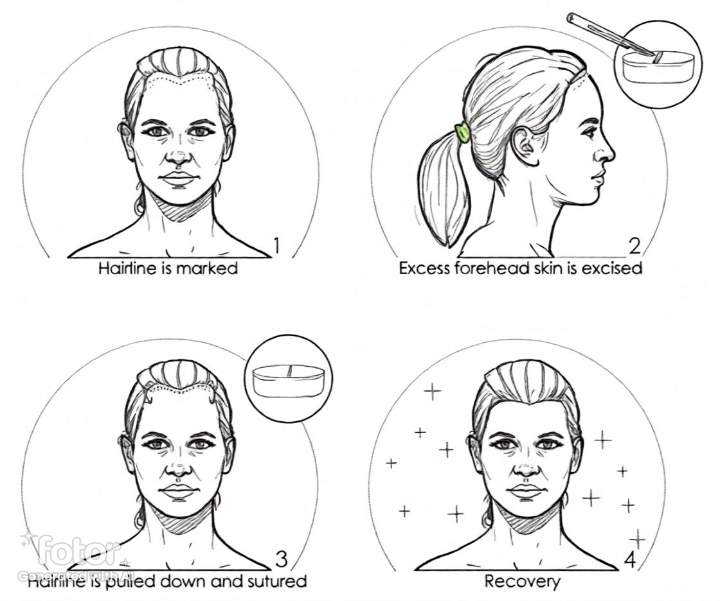
Forehead reduction / hairline lowering
An incision is made along the hairline, a measured strip of forehead skin is removed, and the scalp is advanced forward. A trichophytic closure may help hair grow through or close to the scar, improving camouflage. The amount of lowering depends on scalp laxity and safe closure rather than a fixed number.
Differences in men and women
In many women, the ideal brow may have a gentle arch and sit slightly above the orbital rim, particularly laterally. In many men, the brow is naturally lower, flatter and closer to the orbital rim. Over-elevation in men can create an unnatural or feminised appearance. Forehead reduction is more commonly performed in women; in men it requires special caution because of the possibility of future male-pattern hairline recession.

Preoperative preparation
- Full medical history, medication review and assessment of suitability.
- Standardised clinical photographs.
- Assessment of brow position, eyelid skin, hairline height, scalp laxity and symmetry.
- Discussion of smoking cessation, blood-thinning medication and supplements where clinically appropriate.
- Written consent discussion including benefits, risks, alternatives, limitations and the option of no surgery.
What happens on the day of surgery?
The procedure is usually performed as a planned day-case operation. Depending on the selected technique and patient suitability, it may be performed under local anaesthesia with or without sedation, or under general anaesthesia in some settings. Markings are made before anaesthetic infiltration. The surgeon then performs the planned release, lift, fixation, hairline advancement or skin excision before meticulous closure and dressing.
Dressings, bandage and early recovery
A light head dressing or bandage may be applied to reduce swelling and protect the incision. Bruising and swelling are common in the first one to two weeks. Temporary tightness, numbness, itching or altered scalp sensation can occur. Sutures or clips are usually removed according to the surgeon’s protocol, commonly around one to two weeks depending on the technique.
Postoperative care
- Keep the head elevated as instructed.
- Use cold compresses only if advised, avoiding pressure on the incision.
- Avoid strenuous exercise, bending and heavy lifting during early recovery.
- Follow wound-care instructions carefully.
- Attend planned review appointments.
- Seek urgent advice for increasing pain, expanding swelling, bleeding, fever, wound discharge, visual symptoms or any concern that feels unusual.
Risks and complications
Reported complications vary by technique and patient factors. Peer-reviewed reviews describe issues such as temporary or persistent numbness, visible or unacceptable scarring, alopecia around incisions, asymmetry, under-correction, over-correction, infection, bleeding, haematoma, muscle weakness , delayed healing, skin necrosis and need for revision surgery. Most complications are uncommon, but they must be discussed honestly before surgery.
Limitations and revision surgery
A forehead lift or reduction does not stop ageing, cannot guarantee perfect symmetry and may not replace the need for eyelid surgery, skin resurfacing or non-surgical treatments. Revision may be considered for persistent asymmetry, under-correction, over-correction, scar problems, hairline irregularity or patient dissatisfaction after adequate healing.
MACS Clinic approach
At MACS Clinic, Watford/London, the emphasis is on careful diagnosis, safety, natural proportions, gender-appropriate planning and realistic counselling. The correct operation is the one that matches the patient’s anatomy and concern: brow descent requires a lifting strategy, while a high forehead requires a hairline-lowering strategy.
Summary: Forehead lift = lifts the brow and upper-face soft tissues. Forehead reduction = lowers the hairline and reduces forehead height. They may overlap in selected patients, but they are not interchangeable.
Selected peer-reviewed reading
- Karimi N, Kashkouli MB, Sianati H, Khademi B. Techniques of eyebrow lifting: a narrative review. J Ophthalmic Vis Res. 2020;15(2):218-235.
- Cho MJ, Totonchi A, Guyuron B. Complications in brow lifts: a systemic review of surgical and nonsurgical brow rejuvenations. Plast Reconstr Surg Glob Open. 2018;6(10):e1943.
- Byun S, Mukovozov I, Farrokhyar F, Thoma A. Complications of browlift techniques: a systematic review. Aesthet Surg J. 2013;33(2):189-200.
- Vila PM, Somani AN, Frankel AS. Forehead reduction: a systematic review and meta-analysis of outcomes and complications. Facial Plast Surg Aesthet Med. 2022;24(2):89-96.
- Mauriello JA Jr, Abdelsalam A, McLean I. Endoscopic brow lift: a retrospective review of 628 consecutive cases. Ophthalmic Plast Reconstr Surg. 2004;20(5):322-328.
- Epstein JS, Epstein R. Surgical hairline advancement: patient candidacy and technical considerations. Hair Transplant Forum Int. 2018;28(5):184-188.
Contact MACS Clinic
- Phone: 020 7078 4378
- WhatsApp: 07792 648 726
- Email: enquiries@macsclinic.co.uk
- Website: www.macsclinic.co.uk
- BOOK a FREE Video Consultation: https://calendly.com/macsclinic/free-video-consultation?month=2025-01