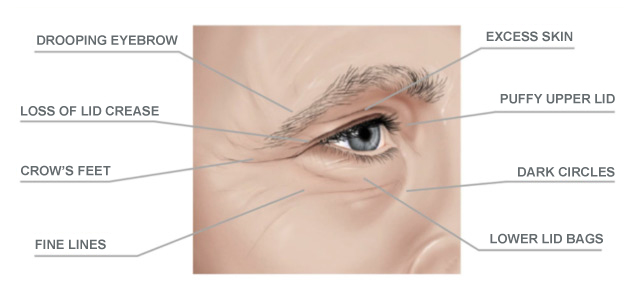
As the forehead ages, the brow position lowers, pushing skin onto the upper eyelid.
This can exaggerate eyelid hooding even when the eyelid itself is normal.
2. How Do We Differentiate:
Excess Skin vs. Eyelid Ptosis vs. Brow Ptosis?
Correct diagnosis is essential for choosing the right procedure.
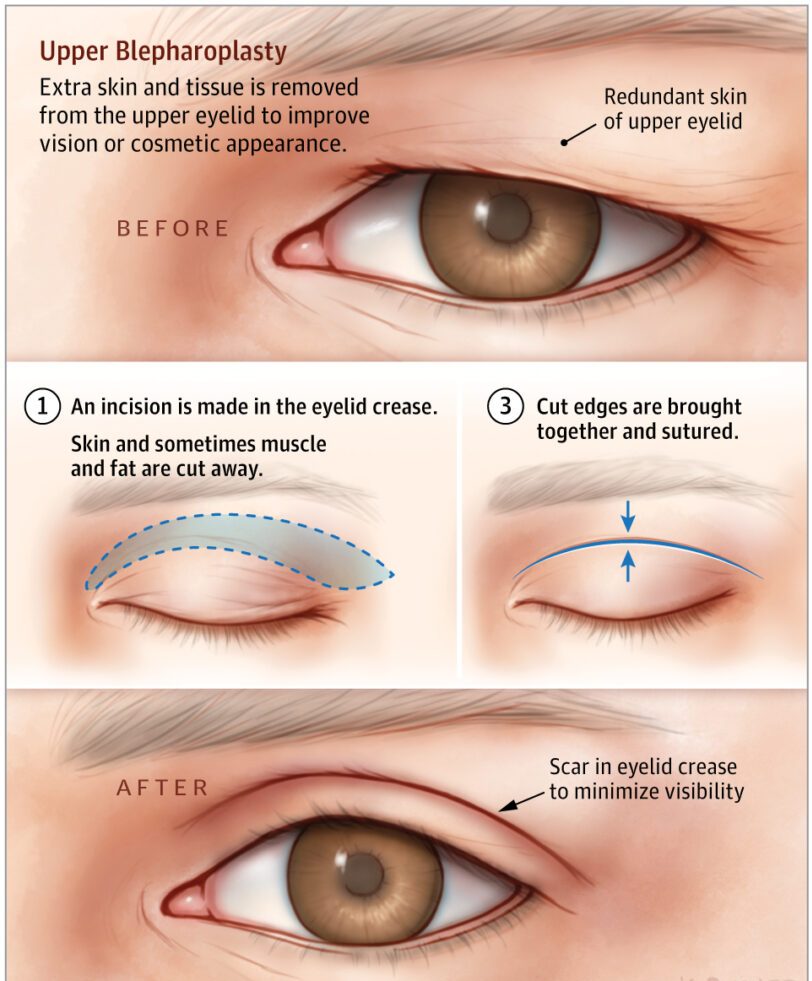
A. Dermatochalasis (Excess Skin)
Redundant skin folding over natural eyelid crease
Eyelid margin height remains normal
Heaviness mainly from skin and soft tissue
Visual obstruction may occur if folds drape over lashes
B. True Eyelid Ptosis
Eyelid margin is low, covering part of the pupil
Typically caused by levator aponeurosis dehiscence
Requires levator repair, not just skin excision
C. Brow Ptosis
Eyebrow sits below its natural anatomical position
Creates appearance of upper-eyelid hooding
Elevating the brow reduces the excess skin fold
May require brow lift rather than blepharoplasty
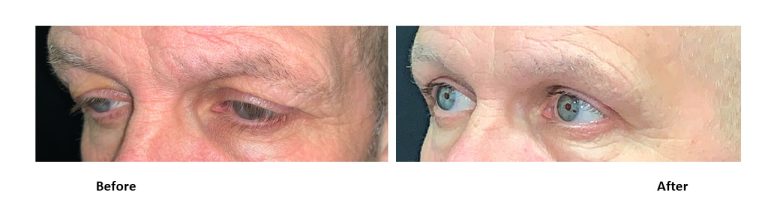
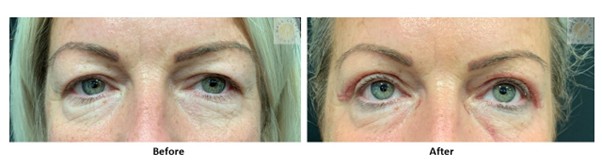
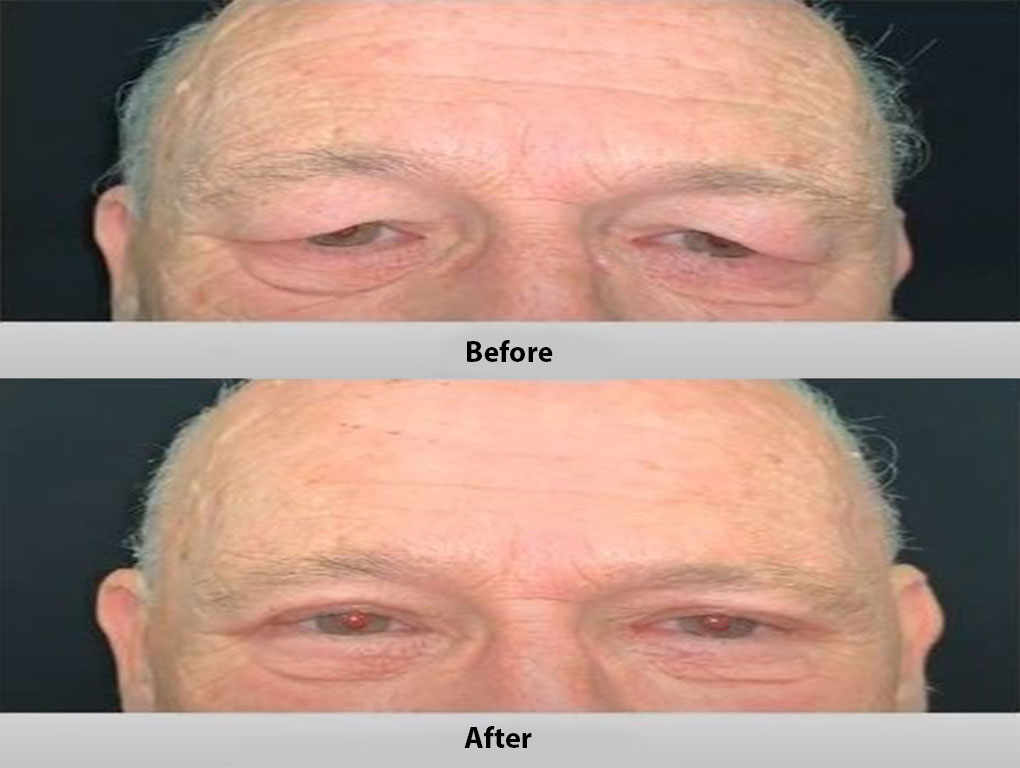
Patient 1: Bilateral Upper Blepharoplasty performed by Mr. Shailesh Vadodaria at MACS Clinic under local anaesthetics
3. Clinical Assessment at MACS Clinic
Our assessment is detailed, structured, and evidence-based.
A. Full Clinical History
Symptoms of heaviness, tired eyes, or visual obstruction
Dry eye history
Contact lens use
Allergies or habitual rubbing
Previous eyelid or facial surgery
B. Precision Examination
Eyelid margin height (MRD1)
Levator muscle function
Brow position and forehead compensation
Skin quality, crease height, fat prolapse
Identification and documentation of pre-existing asymmetry
This is crucial, as some degree may persist post-operatively.
C. Ophthalmic Safety Checks
MACS Clinic advises all patients to undergo:
Visual acuity testing
Intraocular pressure measurement
Optional: visual field analysis if visual compromise is suspected
These are typically conducted by your optician before planning surgery.
D. Clinical Photography
Standardised photographs support:
Accurate diagnosis
Treatment planning
Pre- and post-operative comparison
Medical-legal documentation
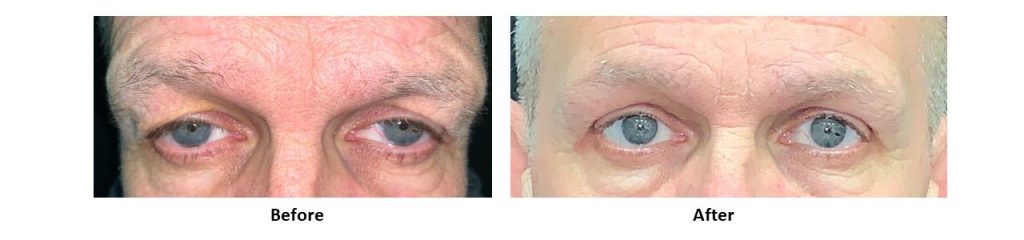
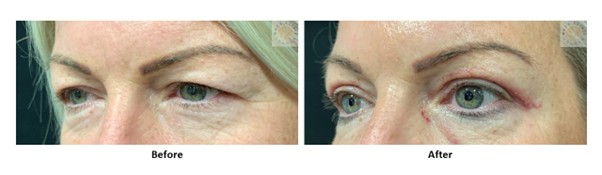
Patient 2: Bilateral Upper Blepharoplasty performed by Mr. Shailesh Vadodaria at MACS Clinic under local anaesthetics
4. Surgical Options for Upper Eyelid Rejuvenation
Every procedure is tailored to your eyelid anatomy.
A. Skin-Only Excision (Conventional Upper Blepharoplasty)
A thin strip of skin is removed along the natural lid crease.
Advantages
✔ Short surgery time
✔ Quick recovery
✔ Restores clean eyelid contour
✔ Excellent for mild–moderate dermatochalasis
Limitations
Does not address muscle redundancy
Does not treat true ptosis
Brow descent may still create heaviness
B. Skin + Orbicularis Oculi Muscle Resection
Used when the muscle contributes significantly to heaviness.
Advantages
✔ More sculpted upper-eyelid frame
✔ Enhances crease definition
✔ Beneficial in thicker, heavier eyelid tissues
Disadvantages
Excessive resection risks hollowing
Slightly longer recovery
Temporary swelling may be more pronounced
C. Supratarsal Fold Repositioning / Levator Aponeurosis Manipulation
Indicated for weak or asymmetric eyelid creases.
Benefits
✔ eye opening may improve
✔ Improves symmetry
✔ May mildly improve eyelid height if levator is lax
This technique is also helpful in Asian eyelid crease creation or enhancement.
D. Fat Preservation or Conservative Fat Debulking
The modern aesthetic principle is:
Preserve volume whenever possible
Remove only truly redundant fat
This prevents a hollow or aged appearance.
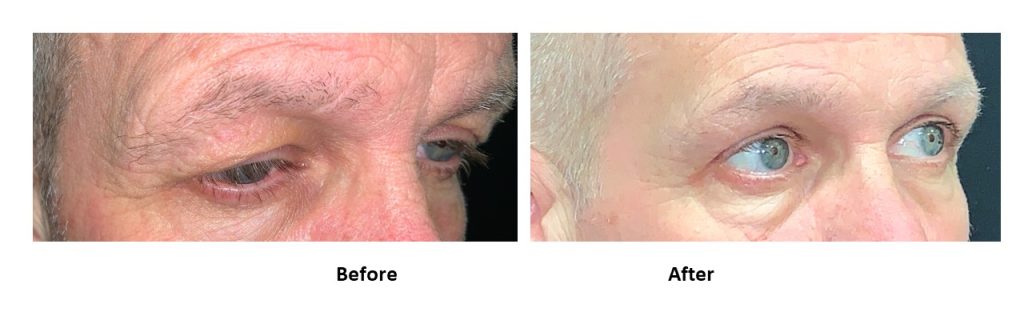
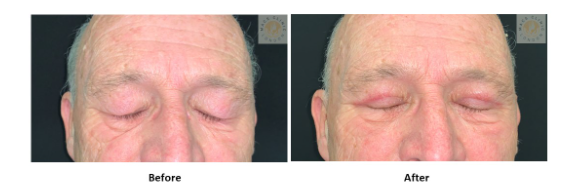
Patient 3: Bilateral Upper Blepharoplasty performed by Mr. Shailesh Vadodaria at MACS Clinic under local anaesthetics
5. Post-Operative Care Instructions
Immediately After Surgery
Apply cold compresses for 48 hours
Keep the head elevated
Use lubricating eye drops and ointment to prevent dry-eye symptoms
Avoid excessive blinking, rubbing, or stretching
Wound Care
Dissolving sutures are used at MACS Clinic
Keep eyelids clean with sterile saline or Clinisept
Makeup should be avoided for 10–14 days
Activity Restrictions
No strenuous exercise for 2 weeks
Avoid contact lenses for several days
Avoid saunas, steam rooms, and dusty environments
6. Possible Risks and Complications
Most are minor and temporary, but patients must be informed.
Bruising and swelling
Mild blurred vision
Watery eyes or dry-eye symptoms
Small areas of asymmetry
Infection (rare)
Scarring (usually well hidden in the crease)
Under- or over-correction, asymmetry
Temporary difficulty closing the eye (lagophthalmos)
Need for revisional surgery
Long-term recurrence due to continued aging
Dry eyes
Blindness (rare)
At MACS Clinic, careful planning and meticulous technique significantly reduce these risks.
Patient 4: Bilateral Upper Blepharoplasty performed by Mr. Shailesh Vadodaria at MACS Clinic under local anaesthetics
7. Long-Term Results & Recurrence
Upper eyelid surgery offers long-lasting improvement.
However, because aging is continuous, some mild recurrence of skin laxity is possible over time.
8. Summary
Excess upper-eyelid skin is both a functional and aesthetic concern. Through a combination of:
thorough assessment,
differentiation between dermatochalasis, ptosis, and brow descent,
safe surgical planning, and
meticulous postoperative care,
MACS Clinic provides natural, refreshed, and long-lasting results for patients seeking upper-eyelid rejuvenation.
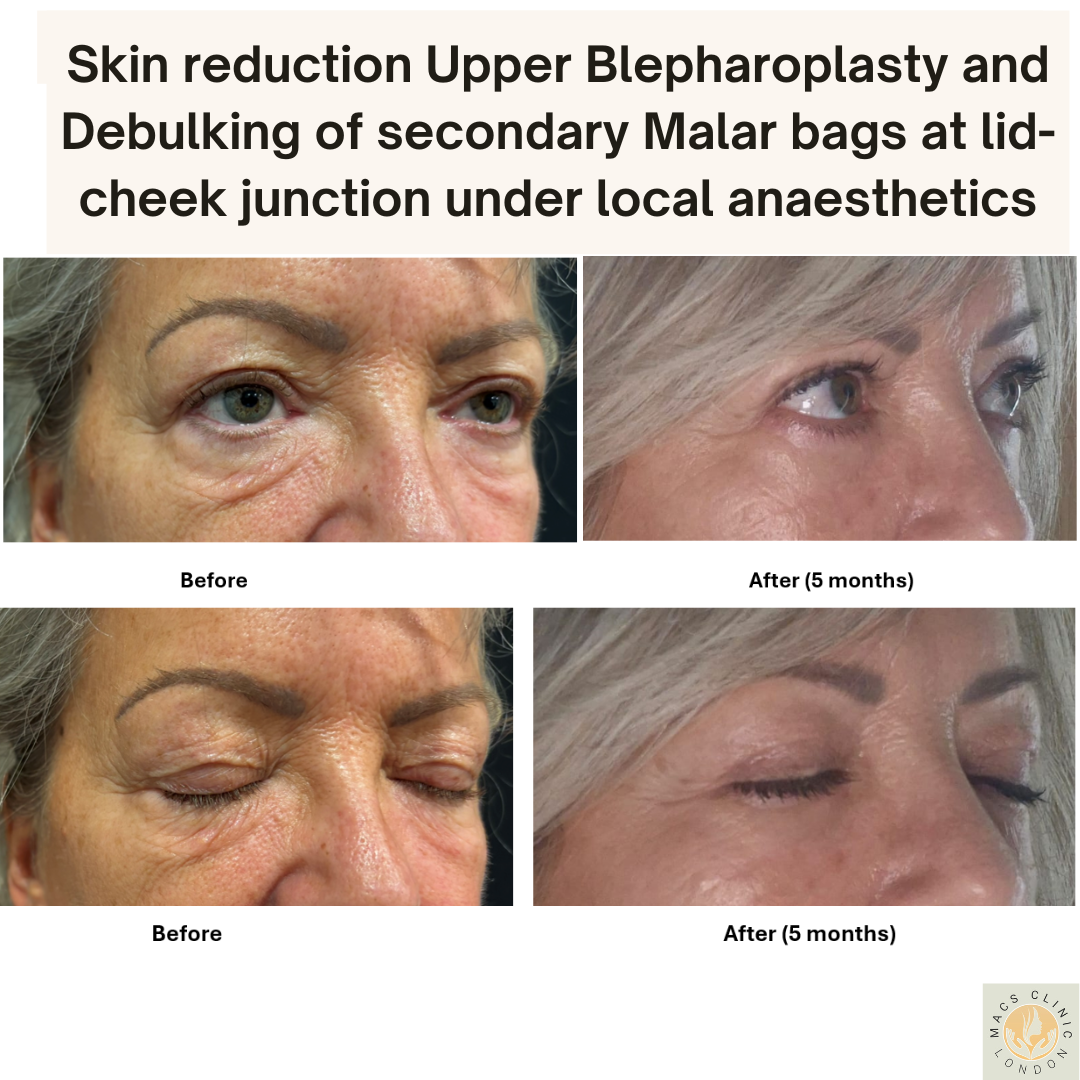
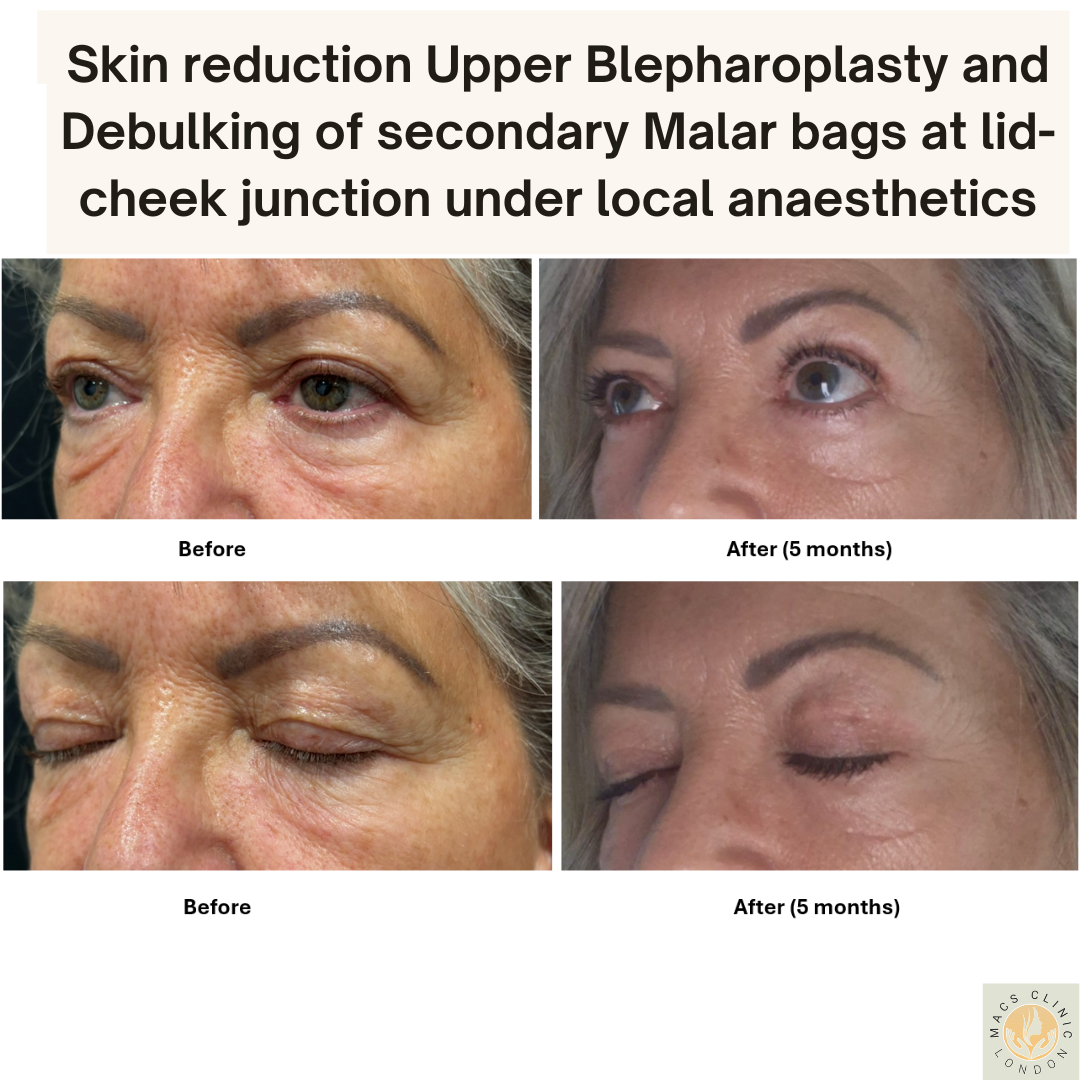
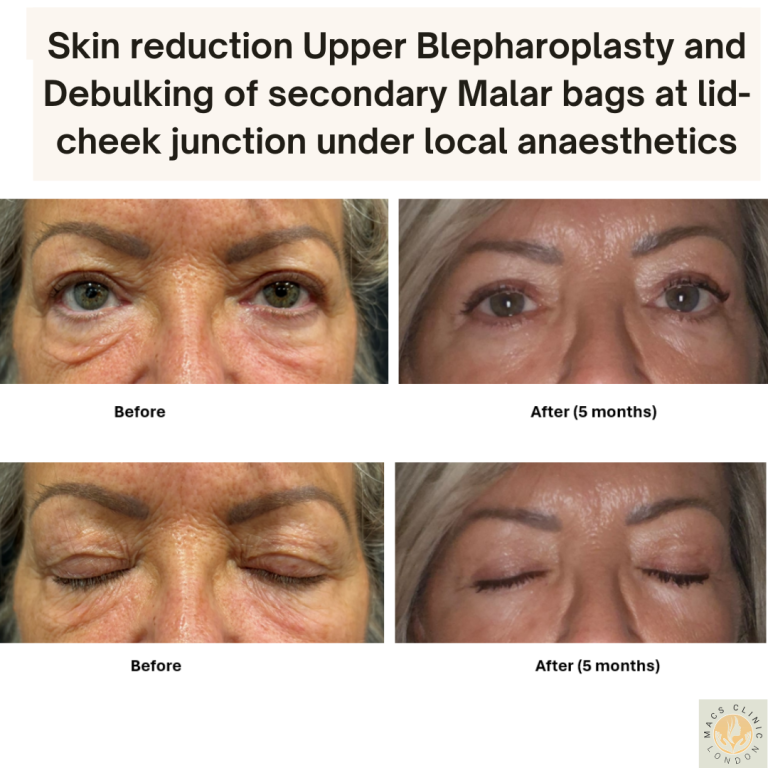
Patient 5: Skin reduction Bilateral Upper Blepharoplasty and debulking of secondary malar bags at lid cheek junction performed by Mr. Shailesh Vadodaria at MACS Clinic under local anaesthetics