Monday - Friday: 9.30 am to 6.00 pm, Saturday - By Prior AppointmentUnit 3, Wilmington Cl, Watford WD18 0AF
Home » News » The Paradigm Shift: How Weight-Loss Medications Are Transforming Body Contouring and Aesthetic Plastic Surgery
The Paradigm Shift: How Weight-Loss Medications Are Transforming Body Contouring and Aesthetic Plastic Surgery
Posted on: 14 Dec 2025
Introduction
In recent years, a remarkable shift in the landscape of aesthetic medicine and plastic surgery has been driven by the widespread introduction and use of new-generation weight-loss medications. Agents such as Mounjaro® (tirzepatide) and Wegovy® (semaglutide) have revolutionized how patients approach weight reduction — offering substantial results through pharmacological means rather than surgery alone.
This revolution has not only changed patients’ body composition and expectations but has also introduced new considerations for plastic surgeons and anaesthetists, particularly in the realms of timing, safety, and peri-operative management.
The Rise of Pharmacological Weight Management
Until recently, sustained weight loss relied primarily on lifestyle modification, bariatric surgery, or older-generation appetite suppressants. The advent of GLP-1 receptor agonists and dual GLP-1/GIP receptor agonists has been a major breakthrough.
These medications — administered as once-weekly injections — promote steady and significant weight reduction by targeting the gut–brain axis that regulates appetite and metabolism.
How Do These Medications Work? – The Mechanism Explained
GLP-1 (Glucagon-Like Peptide-1) Receptor Agonists – e.g. Semaglutide (Wegovy®)
Semaglutide mimics the natural hormone GLP-1, which is secreted by the intestines in response to food intake. It works by:
Suppressing appetite through activation of GLP-1 receptors in the brain’s hypothalamus.
Slowing gastric emptying, making patients feel fuller for longer after eating.
Enhancing insulin secretion and reducing glucagon, leading to better blood sugar control and reduced fat storage.
Dual GLP-1 and GIP Receptor Agonists – e.g. Tirzepatide (Mounjaro®)
Tirzepatide is a dual-acting agent that mimics both GLP-1 and GIP (Glucose-Dependent Insulinotropic Polypeptide). This dual mechanism enhances metabolic regulation by:
Increasing insulin sensitivity and glucose utilization.
Enhancing satiety and reducing caloric intake.
Promoting greater weight loss compared to single-acting GLP-1 drugs.
Agents in Development – Retatrutide and MariTide
Emerging medications like Retatrutide (a triple agonist of GLP-1, GIP, and glucagon receptors) and MariTide (a long-acting GDF15 analogue) promise even more potent and durable results. These next-generation drugs aim to modulate multiple metabolic pathways simultaneously, achieving faster and more sustained weight reduction.
Impact on Aesthetic Plastic Surgery
The increasing use of weight-loss medications is transforming the patient profile in aesthetic and reconstructive practices.
Shift in Patient Goals
Patients who achieve major weight loss medically often seek body contouring procedures such as:
Abdominoplasty (tummy tuck)
Brachioplasty (arm lift)
Thigh lift
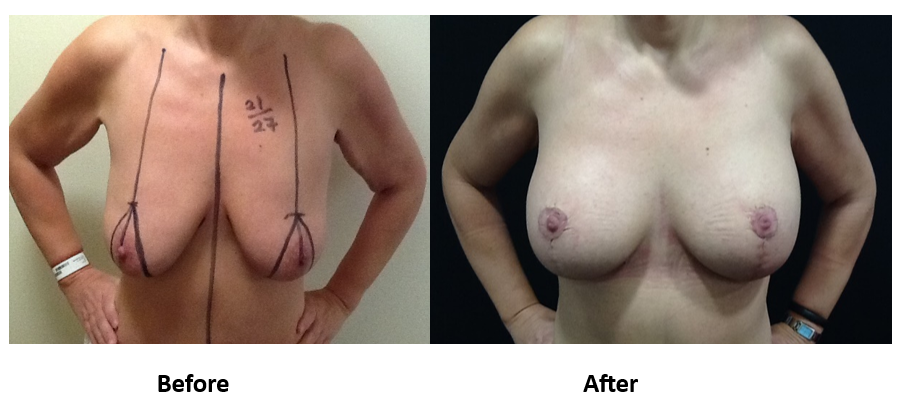
Breast reshaping (mastopexy or reduction)
Lower body lift
While these medications can lead to impressive reductions in body fat, residual skin laxity and loss of tissue volume remain, often prompting patients to pursue surgical refinement.
Patient 1: Liposuction assisted total lower body lift, thigh reduction and brachioplasty following massive weight loss
Patient 1: Liposuction assisted total lower body lift, thigh reduction and brachioplasty following massive weight loss
Patient 1: Liposuction assisted total lower body lift, thigh reduction and brachioplasty following massive weight loss
Patient 1: Liposuction assisted total lower body lift, thigh reduction and brachioplasty following massive weight loss
Patient 1: Liposuction assisted total lower body lift, thigh reduction and brachioplasty following massive weight loss
Patient 1: Liposuction assisted total lower body lift, thigh reduction and brachioplasty following massive weight loss
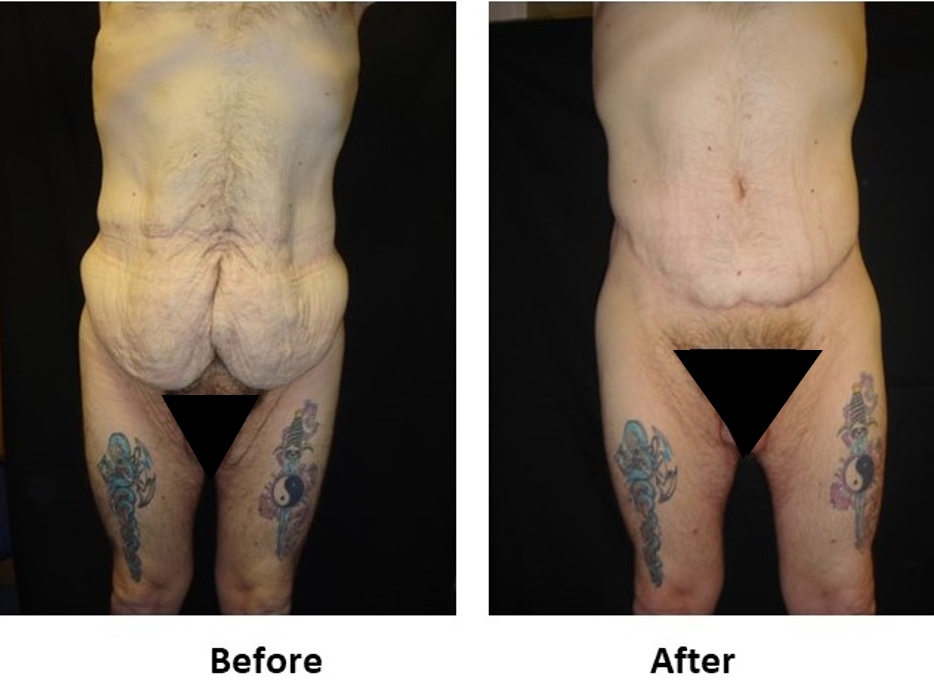
Patient 2 – Abdominoplasty performed in a male patient following post-massive weight loss under general anaesthetics by Mr. Shailesh Vadodaria
Patient 2 – Abdominoplasty performed in a male patient following post-massive weight loss under general anaesthetics by Mr. Shailesh Vadodaria
Patient 2 – Abdominoplasty performed in a male patient following post-massive weight loss under general anaesthetics by Mr. Shailesh Vadodaria
Patient 2 – Abdominoplasty performed in a male patient following post-massive weight loss under general anaesthetics by Mr. Shailesh Vadodaria
Skin and Soft Tissue Changes
Rapid or pharmacologically induced weight loss can lead to:
Deflation of skin and soft tissues without proportional tightening.
Loss of elasticity due to reduced collagen and subcutaneous fat support.
Altered distribution of fat compartments, sometimes in unexpected areas.
This can complicate both surgical planning and aesthetic balance — requiring surgeons to adopt more individualized contouring strategies.
Anaesthetic and Peri-operative Considerations
While these drugs offer major benefits, they also introduce unique anaesthetic challenges that surgeons and anaesthetists must be aware of.
Delayed Gastric Emptying
GLP-1 agonists slow gastric motility, meaning patients can retain food in the stomach even after fasting. This increases the risk of aspiration during general anaesthesia.
Anaesthetic guidelines now recommend:
Withholding weekly GLP-1 medications for at least 1 week before elective surgery (as advised by the American Society of Anesthesiologists, 2023).
Considering longer cessation if symptoms of nausea, bloating, or reflux are present – discuss with your consultants.
Fasting for solids for 24 hours (only clear liquids allowed) before procedure requiring general anaesthesia for patients taking GLP-1 RAs without significant gastro-intestinal symptoms.
We recommend that patients taking GLP-1 RAs with significant symptoms (which includes severe nausea, vomiting and inability to tolerate oral intake) we refer to their prescribing physician for diet and medication modification before proceeding with elective procedures requiring general anaesthesia.
It is reasonable for in-patients to restart GLP-1 RAs and resuming their normal diet.
If you are taking these medications for other than weight loss i.e diabetes, heart conditions then do not stop taking it. Please discuss with your consultants.
Nutritional Considerations
Prolonged use may lead to:
Reduced caloric intake and nutrient absorption, affecting wound healing.
Protein deficiency and vitamin insufficiency, which must be corrected preoperatively.
Fluid and Electrolyte Balance
Patients on weight-loss medications may present with mild dehydration or electrolyte imbalances due to reduced intake — important to evaluate before anaesthesia.
Interaction with Other Medications
Although rare, GLP-1 analogues can delay the absorption of oral drugs, potentially impacting peri-operative medication timing.
Timing Surgery After Weight-Loss Medication
Surgeons should aim to perform body contouring procedures once weight has stabilised for at least six months. Operating during an active weight-loss phase can result in:
Suboptimal skin tightening.
Recurrence of laxity as the body continues to change.
Increased risk of wound complications.
Preoperative consultation should include a detailed discussion of current or recent weight-loss medication use, ensuring close coordination between the surgical, anaesthetic, and medical teams.
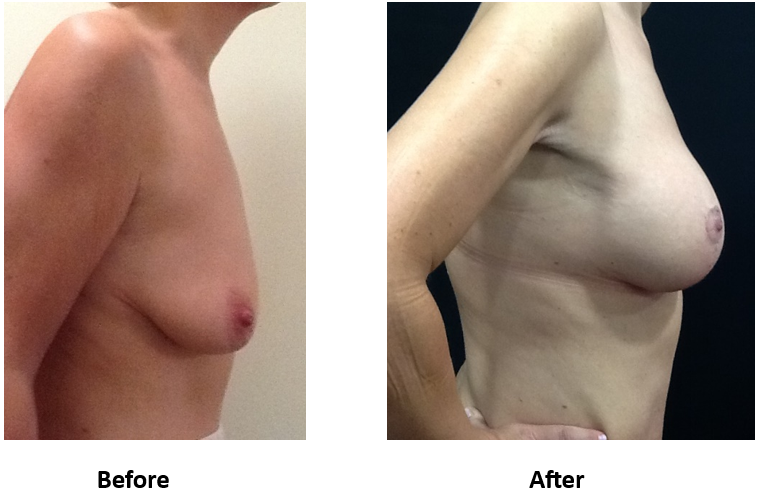
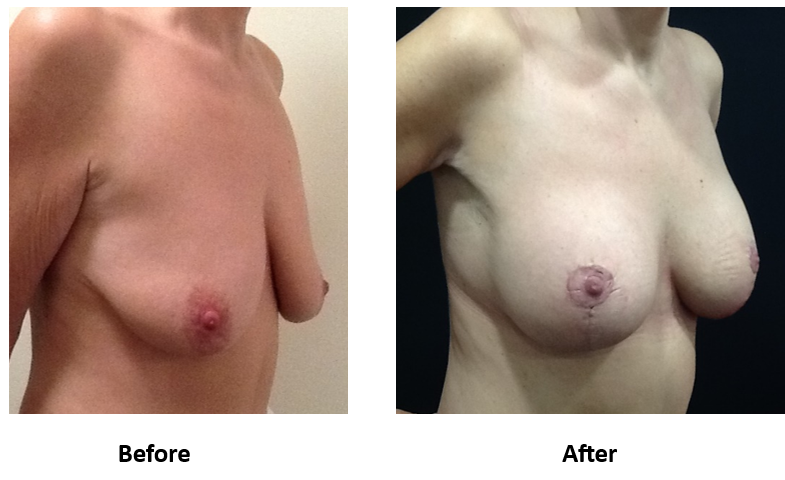
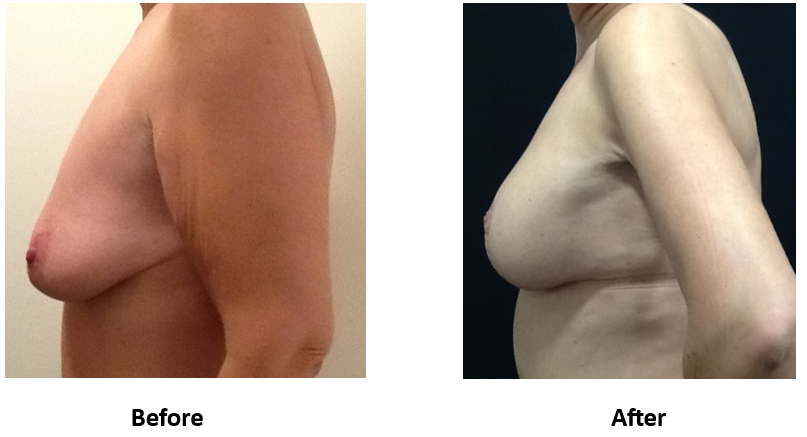
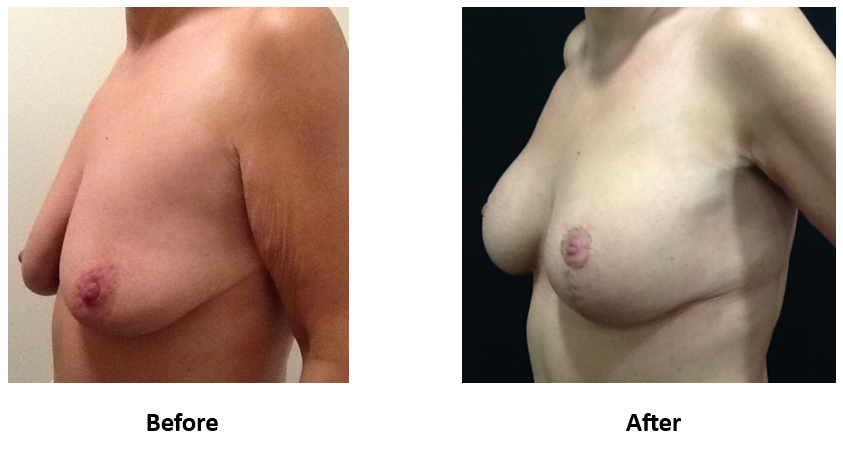
Patient 3: Augmented Mastopexy following post-massive weight loss
Patient 3: Augmented Mastopexy following post-massive weight loss
Patient 3: Augmented Mastopexy following post-massive weight loss
Patient 3: Augmented Mastopexy following post-massive weight loss
Patient 3: Augmented Mastopexy following post-massive weight loss
A New Era of Integrated Aesthetic Care
The rise of pharmacological weight-loss therapy has bridged the gap between medical and surgical aesthetics. Patients can now achieve foundational weight reduction through medications, followed by refinement through plastic surgery once stability is reached.
This synergy demands a multidisciplinary approach, where plastic surgeons, anaesthetists, and endocrinologists collaborate to ensure safety, timing, and long-term aesthetic success.
Conclusion
The introduction of GLP-1 and GIP-based therapies such as Mounjaro (tirzepatide) and Wegovy (semaglutide) has ushered in a paradigm shift in aesthetic medicine.
These agents not only redefine how patients achieve weight control but also reshape how surgeons plan and deliver body contouring procedures. Understanding their mechanisms and effects on anaesthesia is now essential to ensure optimal outcomes, safety, and patient satisfaction in the modern era of aesthetic plastic surgery.